
NeuroFascial Release
By Stephen Myles Davidson, D.O., C-SPOMM
Both DVD’s are taken from the three day NeuroFascial Release Course. We discuss and demonstrate all the material discussed in the NeuroFascial Release Paradigm described below including the Basic Spinal Manipulation Using Inherent Body Forces (Day One of the NFR Course). The DVD’s run about forty five minutes each and clearly depict the physiological and anatomical thinking needed to apply the process.
No information on the DVD’s is intended to replace any medical care. Please see your health professional before using this or any other information.
Please read on for more information about the NeuroFascial Release Paradigm.
Welcome to this brief introduction to the neurofascial release paradigm. Here, we will emphasize its principles as an approach to structural factors in disease.
The paper is divided into five components:
- Definition of neurofascial release (NFR).
- An explanation of how neurofascial release follows osteopathic principles and utilizes a natural phenomenon to normalize abnormal body patterns.
- A glossary of terms and concepts in neurofascial release.
- A description of the process of neurofascial release.
- A treatment approach of spinal scoliosis, using the neurofascial release paradigm, considering cranial, thoracic cage, fascial weakness, and leg length discrepancies in an attempt to describe how one would think about a scoliotic pattern.
Definition: What is Neurofascial Release?
Neurofascial release is a light pressure palpation procedure that uses several inherent body forces. Some of these forces are:
- the hydraulics of the cardiovascular system
- The motility of the central nervous system
- The excursion of the respiratory diaphragm, which applies pressure upon the attached fascial planes continuous throughout the body
- a direct palpatory signal to the physician of increasing vitality when determining the direction of an active correction.
The neurofascial release procedure acts rapidly to normalize structural/functional relationships in the body. It uses a direct palpatory communication between the operator and the inherent healing power of the body, as manifested in fascial response to the physician’s intentful palpation. Like many other osteopathic paradigms, neurofascial release identifies and harnesses a normal, ongoing physiological homoeostatic process and fashions it into a therapeutic tool. It stands on the shoulders of other osteopathic explorers who also discovered how to use a physiological mechanism in a therapeutic way. For example, in the Jones Counterstrain Treatment. Larry Jones, D.O., discovered a way to reset the annulospinal mechanism and thus restore muscle tension. In the Cranial Concept, William Garner Sutherland, D.O., harnessed the therapeutic potency of the CSF, the mechanics of the cranial mechanism and the inherent motility of the CNS in a wonderful series of clinical procedures to diagnose and improve pathological states.
How Neurofascial Release Follows Osteopathic Principles
Disclaimer: It is assumed, in using the neurofascial release paradigm, that all patients have had appropriate medical evaluation and treatment. Osteopathic manipulative treatment, using the neurofascial release paradigm, is then incorporated as a portion of the answer to the patient’s physiological discord. Each case is followed along to the individual’s fullest health potential.
The body works as an integrated whole. Frequently, what appears to be a local problem is, in fact, a local manifestation of a general body pattern. However, only one normal mechanical arrangement exists for the musculoskeletal system to function optimally. The body will continue to function well within tolerances. Outside of tolerances, the system deteriorates and the patient experiences symptoms.
As Andrew Tay1or Still. M.D., D.O., often said (paraphrased), “The normal is always present. It is covered up by abnormal fascial patterns. Seek for the health in the patient.” The goal of applying the osteopathic neurofascial release paradigm is to remove the abnormal and allow the normal, ever present, to operate fully again.
Only direct palpatory patient evaluation provides structural information for treatment. A named disease provides a guideline for physician-physician communication only, but cannot tell how that patient’s unique musculoskeletal history and findings play out to create that symptomology. The objective of neurofascial release, as well as other osteopathic paradigms, is to individualize the care for each patient’s own, unique health-related needs.
The Natural Phenomenon that Neurofascial Release Attempts to Normalize
Neurofascial release can be applied to a wide range at phenomena that we find in the body. Among these are:
- Restrictions in ranges of motion, whether they be active or passive.
- Abnormal spinal mechanics — general, local, or from fascial stress patterns.
- Acute somatic dysfunctions with their attendant tissue changes of bogginess, warmth, moistness, and loss of local elasticity. (If the tissue characteristics return immediately to their pretreatment state after release, evaluate the organ at that level, looking for a viscerosomatic reflex.)
- Chronic somatic dysfunctions with their attendant tissue changes of ropey fibrous tissue, tight muscle, or fascial band within them. They may show evidence of a decreased tissue flexibility and/or dryness.
- Intra-osseous strains within bones as well as strains within the developmental parts. (We will discuss more on this in the Scoliosis Treatment section.)
- Abnormal functioning of the cranial mechanism, such as inadequate excursion, asymmetric or asynchronous motion of cerebral hemispheres; inadequate, scattered, or abnormal cerebral-spinal fluid (CSF) peripheral flow.
- Cranial dural stress band strains and their extensions through the dura to the periphery.
- Sacral abnormality shape, consistency, or positioning between the ilia.
- Constitutional fascial patterns, usually inherited.
- Toxic imprinted patterns from environmental, chemical pollutant exposures.
- Subconscious effects from mental or emotional trauma.
- Fascial flow abnormalities, such as push and pull strains (We introduce and explore these in class). Active fascial stress patterns that push or pull, accompanying structures into abnormal relationships.
- Subconscious operation of mental or emotional forces long after the event has occurred — tissue memory.
- A host of fascial abnormalities may yet be discovered will be amenable to the principle.
- The idea is that there is one normal structural/functional relationship for a body and countless abnormals. Our osteopathic objective is to remove the abnormal parameters and uncover the normal in that patient’s body.
The Process
The process for neurofascial release is very straightforward: For qualitative or general pattern abnormalities, identify and define that parameter. One hand identifies and monitors a parameter. The other hand palpates over the fascia in the direction that causes the abnormal fascial tension to be brought into balance or the abnormal tissue quality or texture to resolve. At the release point, there is a respiratory reaction similar to that seen in a CV4 (compression of the fourth ventricle, a cranial osteopathic procedure). The respiratory rate and depth increases, inhalation-exhalation excursion becomes balanced and equal. This respiratory change follows a global relaxation response, a tissue meltdown if you will, and the re-establishment of a more normal function. CSF (cerebrospinal fluid) may flow fully and rapidly, rostrally to caudally, indicating the treatment is complete.
For example, let’s consider a tissue texture change, such as an acute somatic dysfunction function or global toxicity, or a warp in a bone. We identify the nature of the parameter and apply the NFR procedure while monitoring the parameter. When the release point is palpated, the parameter is changed to normal tissue, tones, and textures. The parameter is then re-evaluated, as is its effect on the rest of the mechanism.
The parameter is a range of motion. The process is to “recruit” the strain, a process we will describe in the Glossary Section. For example, if one is using the arm adduction as the parameter, recruit the strain and seek your release point. When approaching the release point, the tension in the recruited strain lessens. At the release point, the tension disappears and the range of motion increases. Re-evaluate other ranges of motion to determine the effect of releasing the strain globally.
Another way to release individual strains and somatic dysfunction is to evaluate ranges of motion, move the components in the “direction of lifefulness” (See Glossary Section below.) to the end feel, wind the pattern throughout the body and await the release. Re-evaluation demonstrates how effective the process was.
Finally, a key point to remember: Diagnosis in the neurofascial release point paradigm, as in many osteopathic paradigms, is critical. The treatment uses inherent body forces to correct the problem.
Glossary of Terms and Concepts of Neurofascial Release
All osteopathic paradigms explore unnamed physiological phenomena and formulate words to describe them. For example, Larry Jones, D.O., developed the terms “wobble point” and “tender point” to describe his palpatory experiences in the Counterstrain Technique. William Garner Sutherland, D.O., used the terms “point of balanced membranous or ligamentous articular tension” to describe palpatory phenomena unique to the cranial concept. Because Neurofascial Release is a relatively new paradigm, I have similarly created a language to describe and discuss the phenomenon attributed to it. This language also describes how to apply the neurofascial release principles.
Recruit the Strain. Upon reaching an end feel in a range of motion parameter, the physician induces additional tension, moving slightly against the barrier, revealing how the strain extends throughout the body. This recruitment provides a fixed barrier, a fulcrum against which inherent body motions can work. Beginners often do not recruit the strain with enough tension to create this fulcrum. Hence, the body cannot complete the release.
Tissue Speed. When the physician evaluates a range of motion parameter, he/she experiences tissue speed as the rate at which a tissue will smoothly accept the force applied. If the practitioner applies too much force, and the barrier is bypassed, an increasing tissue resistance will be met. The fascial plastic and elastic properties determine the rate of speed at which the parameter can be tested. This often dramatically changes after release.
Release Point. This is a small area that, when palpated, immediately releases the tension and recruited strain or the characteristic of a palpated parameter.
Lock On. When the release point is reached, the body reacts with a little sudden tension followed by a rapid relaxation and pattern reorganization.
Fascial Flow. Fascial motion in any direction, with any force other than the normal expansion and contraction of the cranial mechanism.
Direction of Lifefulness. A palpatory signal when evaluating a range of motion parameter indicating the body’s preference for direct or indirect action treatment. The signal is characterized by an increase in tissue vibrancy and elasticity in the direction of the inherent mechanism’s preference.
Principles of Clinical Examples – Scoliosis
This section provides a rudimentary theoretical approach demonstrating a clinician’s osteopathic thinking in approaching this condition. Many other osteopathic paradigms may lead to the same physiological conclusions. This idea is not all encompassing as, depending on the severity, some scoliosis cases will need other kinds of care including surgical intervention. We assume an initial evaluation reveals a normal, relatively block shape to the vertebrae; the ribs have normal centro- and vertebrocostal articulations with no congenital combining of ribs or vertebrae. What the neurofascial release paradigm does is quickly release the discovered strains. The following four examples demonstrate a use of neurofascial release:
The shape of the skull:
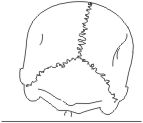 If the shape of the skull causes one side of the occipital bone or the condyl to be lower than the other side, the patient will tilt the head to the opposite side. This is because of the righting reflex and the need for the eyes to try to stay on level with the horizon. Subsequently, the patient will raise one shoulder and the opposite hip. Thus is created a functional scoliotic curve. The curvature is the normal consequence of the body working around a mechanical abnormality.
If the shape of the skull causes one side of the occipital bone or the condyl to be lower than the other side, the patient will tilt the head to the opposite side. This is because of the righting reflex and the need for the eyes to try to stay on level with the horizon. Subsequently, the patient will raise one shoulder and the opposite hip. Thus is created a functional scoliotic curve. The curvature is the normal consequence of the body working around a mechanical abnormality.
In evaluating the cranium, we need to determine if this strain, resulting in the occipital condyle’s unleveling, is created locally by cranial dural stress band strains, an incompletely expanded cranial mechanism on one side, or perhaps peripheral tensions from nerves imbedded distally in the fascia. We discover those patterns that resulted in the local cranial shape abnormality and release them.
Thoracic rib cage imbalance:
 The rib cage’s elastic recoil tends toward exhalation. The expansive forces of the lung oppose this, so that a balance exists between the two. One side of the rib cage may become less expanded than the other from increased rib cage elastic recoil or decreased expansive lung forces. Depending upon how that strain plays out, a curve towards or away from that side occurs.
The rib cage’s elastic recoil tends toward exhalation. The expansive forces of the lung oppose this, so that a balance exists between the two. One side of the rib cage may become less expanded than the other from increased rib cage elastic recoil or decreased expansive lung forces. Depending upon how that strain plays out, a curve towards or away from that side occurs.
With hands bridging the anterior axillary line to the posterior axillary line in the middle of the rib cage, compare the relative size of the left and right rib cage sides. Experience how each side of the thoracic cage feels in your hand. In the picture, the left side of the thoracic cage is narrower, shorter and less expanded than the right side.
To treat, palpate the boundary between the compressive thoracic wall forces and the expansive lung tissue. Release this area, using neurofascial release.
Many times, dramatic and immediate straightening of the spine occurs as the thoracic cage expands. In long-standing thoracic cage straits, perhaps of decades, it may take months of repeated treatment for a soft tissue remodeling to occur.
Sacral base unleveling from an anatomical short leg:
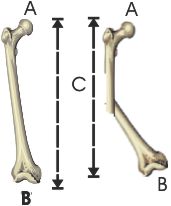 A cause for an anatomical short leg is a warp within the long bones (tibia, femur, fibula). In the picture above, the distance from the head of the femur to the condyls along the shaft of the bones is the same (A to B). A warp in right femur bone makes that bone’s length ( C ) shorter. Use the NFR paradigm to release the tissue forces creating warp and shortened distance, restoring the normal leg length. Another warp creating a short leg may originate in the intraosseous strain of the innominate’s developmental parts.
A cause for an anatomical short leg is a warp within the long bones (tibia, femur, fibula). In the picture above, the distance from the head of the femur to the condyls along the shaft of the bones is the same (A to B). A warp in right femur bone makes that bone’s length ( C ) shorter. Use the NFR paradigm to release the tissue forces creating warp and shortened distance, restoring the normal leg length. Another warp creating a short leg may originate in the intraosseous strain of the innominate’s developmental parts.
Some scoliotic curves are the person’s adaptation to a generalized tissue toxicity from chemical pollutant exposure. A chemical exposure has imprinted a weakness in the general fascial system. No chemical may remain in the tissues, but its physiological effect continues. In the same way, many patients will say, “Ever since I had this infection, I’ve felt such and such…” Obviously, the infection state has long passed, but the infection created an effect that is maintained in the system, running like a computer software program.
The weakened fascia is not as able to hold the body upright with a straight spine against gravitational forces. Like a slightly deflated animal balloon that loses its shape, the spine curves. Immediate removal of this fascial imprint “blows up the balloon” (allowing the free, unfettered flow of the life force in the fascia) restores the normal spinal curvature.
Other factors to consider in scoliosis are leg length discrepancies from unequally arched or flat feet and desiccation of cartilage at the knee or femoral-coxal joints. All of these can change the leg length with resultant sacral base unleveling and spinal scoliosis. First diagnose, then treat, using the neurofascial release paradigm to quickly normalize the structural problems. As in all osteopathic treatments, cases are followed along to their full potential conclusion.
Clinical Examples and Testimonials
Dr. Davidson has made a profound change in our daughter’s life.
She has Chronic Fatigue Immune Dysfunction Syndrome and Fibromylgia. She also had a rather severe scoliosis and unstable very low blood pressure. She was only able to take about two courses in college per semester and was able to do very little else. By the end of her undergraduate work she was going full time and has just finished her first year in Law School – full time and in another state.
Dr. Davidson corrected the severe scoliosis in her lower back on her first visit and his work on her neck and skull has given her a stable blood pressure and MUCH more energy.
Dr. Davidson’s manipulations along with the medications she takes have given her back a full life. Dr. Davidson has really helped other members of my family as well, when they had injuries or chronic conditions.
I recommend him very highly.
K. R. Glendale, AZ
I wanted to let you know that I noticed many good effects from your treatment right away — this breathing in two lungs is of course really great! Yesterday – on our last warm day here – I painted my front and back porches and still had energy to spare, pretty unheard of for me – and as sore spots started complaining later in the day, I put my hand on whatever I could reach and found release points and woke up this morning not sore from the painting at all – now, that’s REALLY unheard of!
When I left Steve’s office the first thing I noticed was that my distance vision was distinctly better – I could see sharp outlines on the leaves on trees again! Very beautiful, thank you so much… And colors seemed richer though that’s harder to be sure of. I went shopping this evening and forgot my reading glasses – but I could read labels, by squinting to be sure but it would have been impossible before.
For the better part of a year now when I go to switch lanes on the highway I check at least 4 times, very frustrating, my rational brain knows that I saw what I needed to see the FIRST time! Now I’m switching lanes in a much more normal fashion – that uncertainty or lack of processing, and feeling of alarm are much abated. I stopped in at David Burns’ office to see Bob Mastrianni and he had me sit in on T.G’s treatment — and she was saying the SAME things about highway driving and how it had changed!!!!
There are more subtle changes in other OCD [symptoms] — I’ve worked with that in other ways that have helped too, but there was a significant good change after my appt with you.
David remarked about my vision because he could see the change in my eyes, and the lack of strain and good new color in my face. Like many other middle-aged women I have some feeling about the changes in my skin, weight, and hair but they don’t bother me very much. What I’ve really felt though, is that for the past number of years when I look in the mirror it’s been sad to be looking at ‘old-woman’ eyes – that’s partly a too-much-sympathetic problem but also there’s been a lack of luster – and now there’s a good shift back – thank you, thank you.
I’m getting used to having nice color in my face, and to having shoulders that are closer to level with each other. My right shoulder has been down since I was 11 years old! (when I had an episode of torticollis – happened in the middle of a school day, nasty and took the better part of a week and a whole lot of hot packs to resolve very much – ever since the problem has been identified as a high left shoulder, not a dropped right one. Sorry there were things I forgot to tell you, including a couple of broken bones – so many body parts, so little time!) Think that might explain a few things??? I tried Fulford’s arms-out breathing exercise [Hanging Arm Exercise from The Twig Unbent] (which always felt so awful to do that I had long ago given up) — and what a lovely experience to have it feel GOOD to do!!
SC, Connecticut
Conclusion
Neurofascial release identifies and accesses a normal, ongoing homoeostatic process. Like so many osteopathic paradigms of the past, NeuroFascial Release fashions the physiological phenomena into a therapeutic tool. We hope you will explore the NeuroFascial Release concept and find it to be an exciting and creative addition to your already effective osteopathic therapeutic regimen.